
Why do people continue to smoke despite knowing its associated health risks?
By Lola Kommineni, July 2026
Introduction:
In 2025 the National Centre for Epidemiology and Population Health in Australia declared that smoking causes 24,000 deaths nationwide each year, accounting for 66 deaths per day. Smoking is deemed socially unacceptable in society, and this is clearly reflected in our everyday lives, whether it’s through no smoke zones or grotesque imagery found on cigarette boxes. Over the last century, smoking went from a glamorized activity that displayed high social status and wealth, to a widely discouraged activity that is looked down upon. And this begs the question: when smoking is considered such a harmful activity, why do people continue to engage in it? What makes quitting, or avoiding smoking so difficult?
How smoking negatively impacts heart health
To begin, it’s important that we discuss why smoking is considered such a risk to cardiovascular health. Whilst there is a plethora of ways that smoking harms the heart, here are the most significant and common ways.
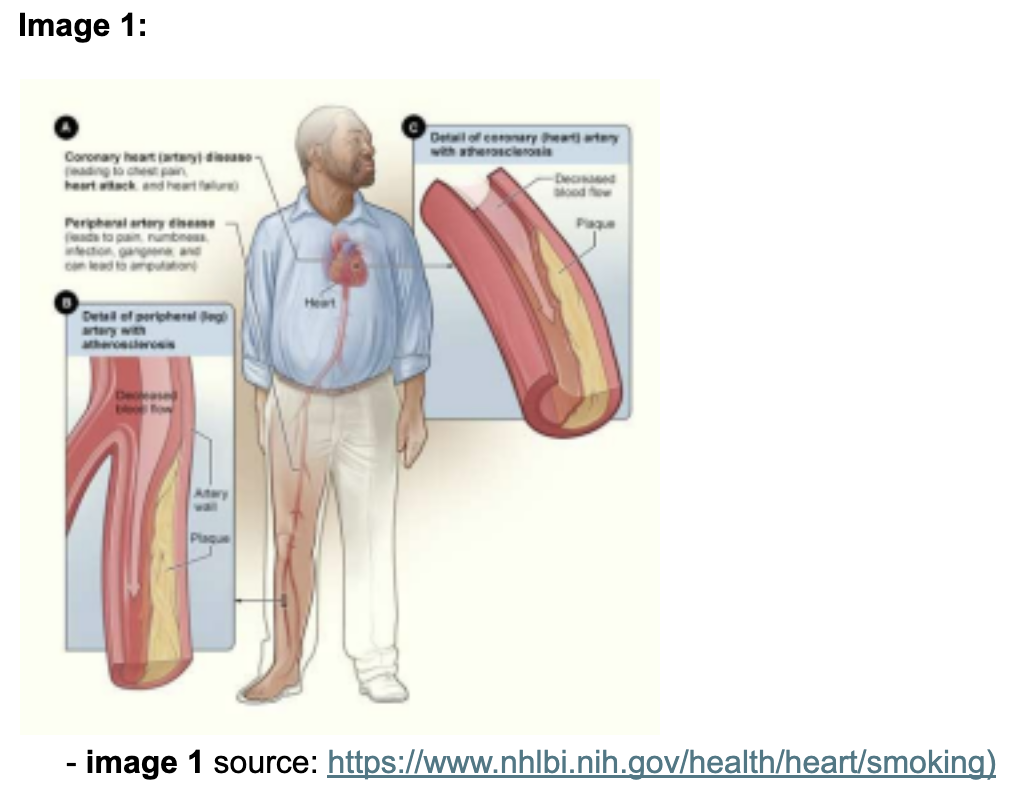
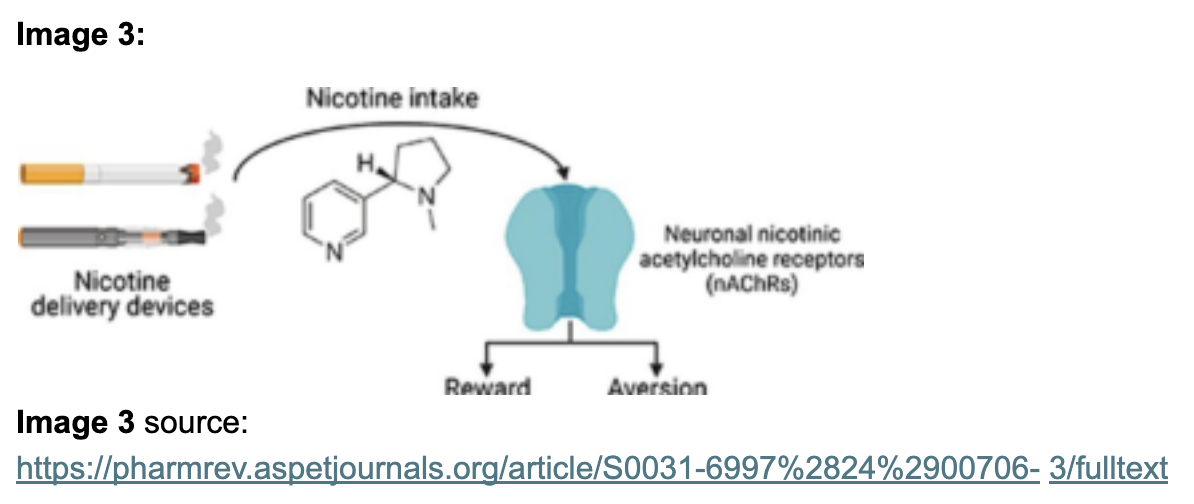
Cigarette smoke contains a wide range of chemicals and gases, many of which can be toxic. When cigarette smoke is breathed in, the chemicals in it travel through the nasal cavity and pass across the alveolar membranes in the lungs, diffusing into the blood stream. These chemicals can damage and irritate the walls of arteries, which are the blood vessels that deliver oxygenated blood from the heart to foreign tissues in the body. This can cause them to become inflamed, increasing the likelihood of plaque building up and hardening on the arterial walls. As seen in Image 1, this has major implications for blood transport, as this can cause arterial walls to become narrower and smaller, which characterises a condition known as atherosclerosis. Therefore, blood flow to certain organs can be restricted. This can lead to heart complications such as coronary heart disease, which is where the arteries delivering oxygenated blood to the heart are blocked. This can lead to myocardial infarction (heart attack), which can be fatal. Figure 1 illustrates how smoking is seen to exacerbate the risk of developing atherosclerosis.
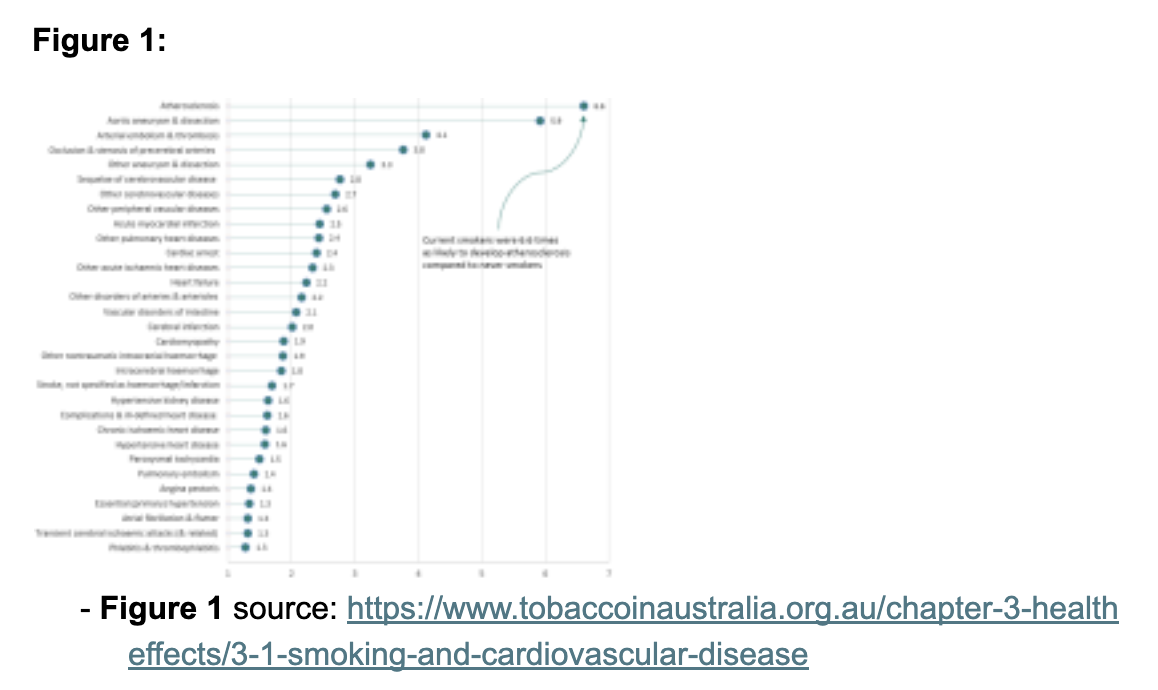
Furthermore, carbon monoxide is a component of many cigarettes. It is a toxic gas that is commonly used in vehicle exhausts and gas stoves, as well as tobacco smoke. When it has entered the blood after being inhaled from cigarette smoke, it can take the place of the oxygen found on haemoglobin in red blood cells which is depicted in image 2. This effectively reduces the quality and quantity of oxygenated blood that reaches heart muscles, meaning that a higher volume of blood is required to deliver adequate amounts of oxygen to the heart to support cardiovascular function.
Tolerance vs dependance:
To unpack why individuals engage in smoking despite its harmful effects, we need to understand the foundational concepts of tolerance and dependence. Tobacco smoke contains nicotine, which is a legal drug that is classified as a stimulant. According to the alcohol and drug foundation of Australia, “Stimulants are a class of drugs that speed up messages travelling between the brain and body. They can make a person feel
more awake, alert, confident or energetic.” Therefore, individuals can become tolerant of smoking and dependent on smoking.
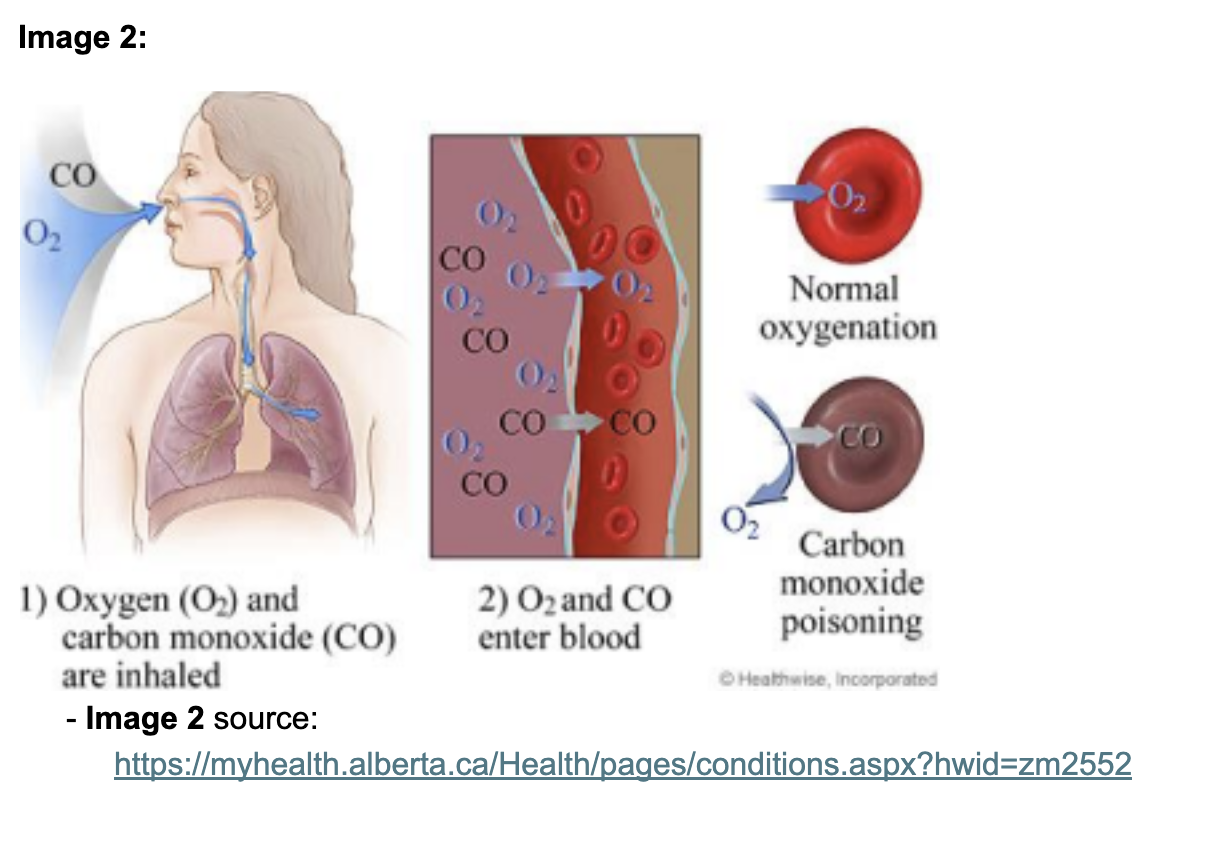
Nicotine acts on a diverse subtype of receptors found throughout the Central and Peripheral Nervous System, called the Nicotinic Acetylcholine receptors as seen in image 3. This initiates the release of neurotransmitters such as dopamine, which can create feelings of pleasure, stimulation, and help modulate one’s mood.
Tolerance is characterised by the body progressively requiring a larger dosage of nicotine overtime, to achieve the same stimulation from smoking. Tolerance can develop due to the neuroadaptation that occurs from repeated and regular exposure to nicotine. Therefore, during prolonged nicotine usage, the body initiates responses to nicotine at an increasingly lower magnitude. This explains why individuals who smoke one cigarette per day can progress overtime to smoking more than ten cigarettes per day. It has also been observed that for this reason, chronic smokers experience effects of smoking such as nausea or dizziness to a lower degree compared to non-smokers, when given the same dose of nicotine.
Dependance on the other hand is characterised by experiencing symptoms such as headaches, anxiety or restlessness when abstaining from tobacco. This indicates the reliance that the body has developed on nicotine. Therefore, many individuals continue to smoke and find quitting a difficult prospect despite their potential awareness of its negative health impacts. For many chronic smokers, smoking becomes a habit to avoid withdrawal rather than to feel pleasure or stimulation due to the body’s tolerance of the substance.
Withdrawal and Relapsing:
Withdrawal symptoms can also include irritability, reduced quality of sleep, and even depression as well as the negligence of social and recreational activities to make time for smoking and are worsened by severe cravings for tobacco. These symptoms tend to increase until their peak at around a week after quitting smoking and declining over 2 or more weeks of abstinence. Therefore, withdrawal symptoms cause a large percentage of the smoker demographic to relapse and return to old smoking habits.
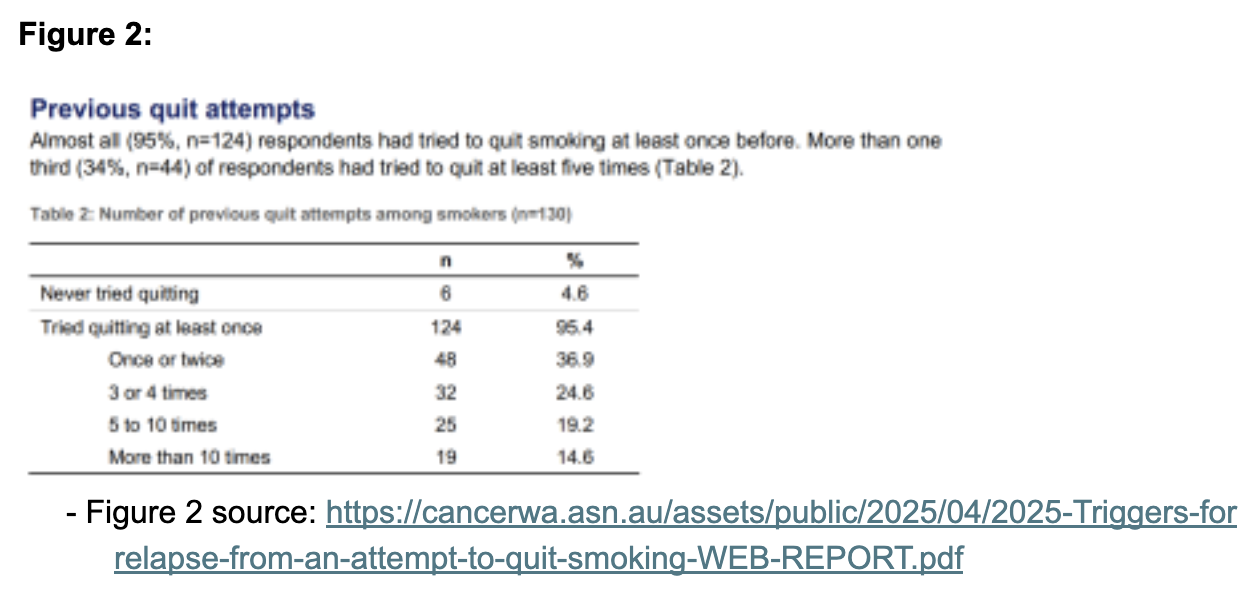
A relapse occurs when an individual stops maintaining their goal or abstaining from or reducing usage of tobacco and nicotine. A study conducted amongst Australian smokers depicted the number of times that individuals had tried to quit smoking and had eventually relapsed which is shown in figure 2. Furthermore, a study referenced in “Drugs and behaviour: An introduction to behavioural pharmacology.” By McKim W and Hancock S” also suggests that the severity of withdrawal is unrelated to smoking frequency or length of smoking history, rather related to withdrawal symptoms from other drugs of abuse. As a result, avoiding the behaviour of smoking can be considered subjectively difficult for many who have a status of smoking.
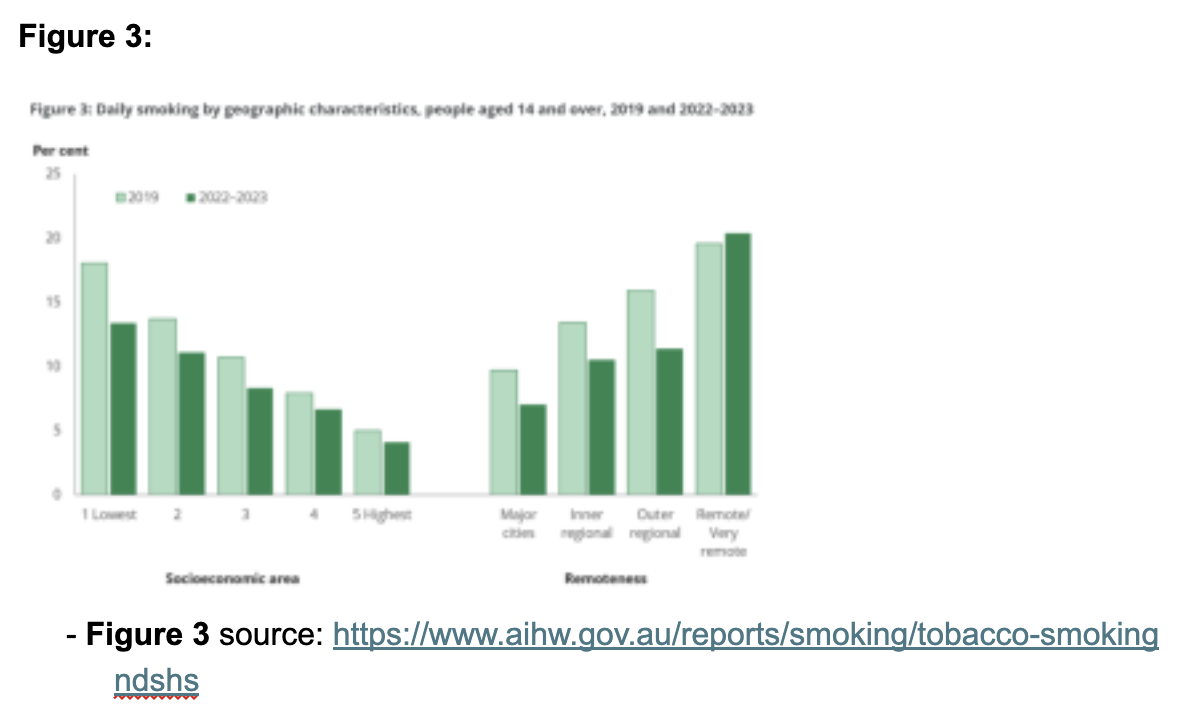
Finally, smoking is often used as a coping mechanism to relieve stress or anxiety due to its stimulative and pleasure inducing effects at a neurochemical level. A study called “Associations between smoking to relieve stress, motivation to stop and quit attempts across the social spectrum: A population survey in England” found it to be plausible that a belief that smoking reduces stress can undermine intentions to quit smoking, and can reduce one's willingness and motivation to quit smoking. This idea is evident in the demographic of low socioeconomic status (SES) which typically experience lower access to income, employment, and education. Those of Low SES, particularly those who were homeless, were observed to have a higher prevalence of smoking, due to high levels of financial stress, which is seen in figure 3. However, this could also be explained by the low levels of health literacy amongst the demographic, which indicates a general lack of understanding of smoking and its negative health impacts. This could have also contributed to low levels of motivation to quit and subsequently abstain from smoking permanently.
This Article is written by our volunteer student research team at Feel Every Beat, and is intended for educational purposes only. It is not a substitute for professional medical advice.
BIBLIOGRAPHY:
- https://www.nhlbi.nih.gov/health/heart/smoking
- https://www.tobaccoinaustralia.org.au/chapter-6-addiction/6-11-tolerance dependence-and-withdrawal
- https://www.health.gov.au/our-work/tobaccofacts/smoking-and-heart attacks?language=en
- https://pmc.ncbi.nlm.nih.gov/articles/PMC9113576/
- https://nceph.anu.edu.au/news-events/news/australias-biggest-killer-smoking causes-66-deaths-every-day-and-24000-year
- https://www.heartfoundation.org.au/your-heart/smoking-and-your-heart - https://adf.org.au/drug-facts/stimulants/
- https://www.sciencedirect.com/science/article/abs/pii/S0002934308001034
- https://myhealth.alberta.ca/Health/pages/conditions.aspx?hwid=zm2552 - https://adf.org.au/reducing-risk/relapse/
https://www.who.int/europe/news/item/29-09-2020-tobacco-use-and-exposure to-second-hand-smoke-linked-to-more-than-20-of-deaths-from-coronary-heart disease